
[Research] Heart rate variability in physiological and pathological conditions
Sabah Hammoud's doctoral thesis

This week I was part of the committee evaluating Sabah Hammoud's doctoral thesis, heart rate variability in physiological and pathological conditions. The Ph.D. defense was here in The Netherlands, at Radboud University, and the work was carried out between the Radboud University Medical Center and the Lebanese University in Beirut, Lebanon.
I want to first thank Professor Mazen Kurdi and Sabah for involving me in the examination committee, Professor Bart van den Bemt for inviting me to and congratulate Sabah again for her excellent work and great discussion during the defense.
Here I’d like to provide a few pointers to her papers (most of the thesis has already been published in peer-reviewed journals), as I think there are quite a few interesting findings in there.

Sabah’s work covered a very broad range of topics, including psychological stress (university exams), steroid use, and fasting during Ramadan in healthy and hypertensive individuals.
Most of the studies had a longitudinal design and data collection was carried out in free-living, hence in realistic conditions, outside of the lab. I want to stress that this is not easy work to do, and is not easy to get it published either, as most of the HRV world has a bit of an outdated view of these things (i.e. requiring data collection in the lab, when it is as far as possible from real life….).
Anyways, among the many papers published, the ones that I found the most interesting personally were the university exams study, looking at the impact of psychological stress before, during, and after the exams, and the fasting during Ramadan studies, looking at meal timing and fasting and its relationship with HRV.
During my discussion with Sabah most of my questions were linked to these topics, and in particular to some of the differences she found in heart rate and HRV metrics in response to psychological stress, as well as some of the differences between her work on fasting and published literature.
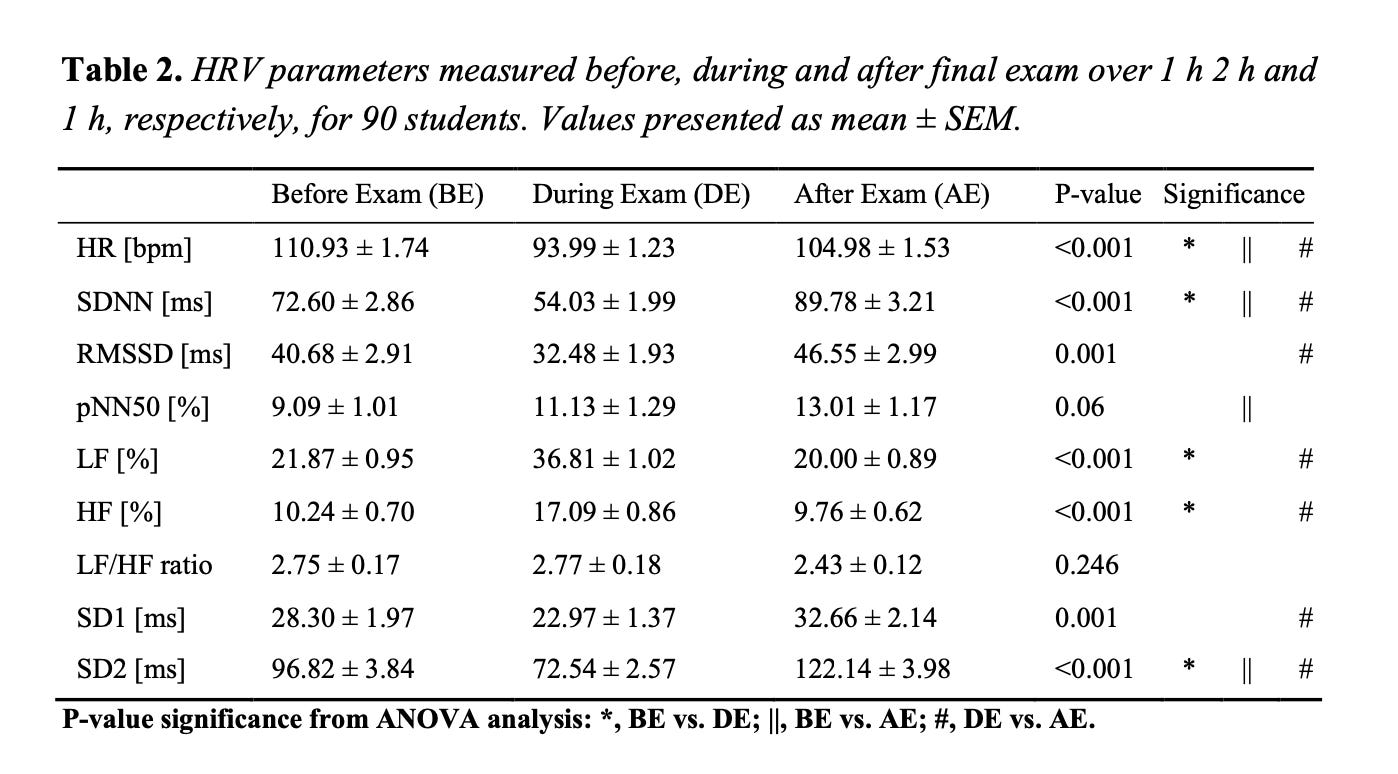
When it comes to psychological stress, Sabah highlighted how only HRV was able to capture the higher stress typical of exam settings, which was not shown in heart rate. This is in line with my experience as well: we use HRV as it is a more sensitive marker of stress, it captures stress in ways heart rate alone cannot. There’s a lot more in the paper, in terms of various analyses and stratifications based on students’ characteristics and perceived stress levels, please see the full text below if interested.
Stress and Heart Rate Variability during University Final Examination among Lebanese Students. Paper here.
The studies on fasting during Ramadan did not show any baseline change in HRV. This was at first somewhat surprising, as much of the literature on fasting seems to show a reduction in heart rate and HRV. However, this difference could be due to the fact that during Ramadan the goal is not weight loss, which is typical of other fasting studies, and therefore the main reason behind the different outcomes in these studies could be (lack of) caloric restriction. Sabah did not measure caloric intake or expenditure, but she confirmed that typically during Ramadan meal timing is different but the amount of food and even the number of meals is similar to other periods of the year, and therefore does not lead to caloric deficit. I personally experienced quite some changes in resting heart rate and HRV last year when I consistently lost weight, and since then I have become more interested in learning more about these relationships. See the studies below for more information.
Effect of Ramadan Fasting on Heart Rate Variability as a Measure of Cardiac Stress in a Lebanese Cohort. Paper here.
Impact of Fasting on Cardiovascular Outcomes in Patients with Hypertension. Paper here.
Impact of Ramadan Intermittent Fasting on the Heart Rate Variability and Cardiovascular Parameters of Patients with Controlled Hypertension. Paper here.
During our discussion, we then moved to broader topics in the context of the applied use of heart rate variability. In particular, there are two important points that I think we still struggle with: chronic effects and screening based on cutoff values.
When we carry out HRV studies, we often look at acute stressors. Acute stressors have a large, immediate effect, on our physiology, and as such, we can typically easily capture them with HRV measurements. However, seeing a certain acute effect, does not necessarily mean that we have the same chronic effect. A simple example here is exercise: acutely, exercise is “bad”, HRV is suppressed, and all sorts of health markers look like we are not doing particularly well. However, chronically, exercise will lead to improved health. While exercise is an obvious example, we cannot know if other stressors act similarly (e.g. university exams or diet). This is one of the reasons why I am “opposed” to continuous (meaning 24/7) HRV analysis and how it trivializes these complex relationships. We cannot assume that an immediate acute suppression in HRV means negative stress, we need to assess stressors in a certain context (e.g. first thing in the morning, far from the stressor itself, to determine the body’s response). See also this blog. Talking with Sabah about these topics, she also acknowledged the difficulties and proposed to look longitudinally in the long term at the effect of these stressors, which I think is indeed pretty much the only thing we can do, given that we cannot extrapolate from acute responses to chronic ones.
The second point of our conversation on cutoff values and screening was interrupted by the end of the discussion (in The Netherlands we have exactly one hour, not a second longer). Here the issue at hand is how can we include using HRV in medical practice, given its relevance in our health, but without reference values or tables the way we do for example for blood pressure or other markers. Personally, I do not think that this is really possible, given the very broad range of HRV values we can find even among a very homogeneous sample of people. Maybe we can still do some macro stratifications, but genetics here plays an important role, and I would find it difficult to make any claims given a person’s absolute HRV values. I discussed this in more detail in my article about low HRV, here. I do not have a solution, but my current view is that HRV is a more useful tool in the context of assessing relative changes over time, in response to various stressors, and not as much as a way to stratify individuals, even though this is how we tend to think, in medical terms.
Alright, that’s all for this blog. Congratulations again, Sabah.

Marco holds a PhD cum laude in applied machine learning, a M.Sc. cum laude in computer science engineering, and a M.Sc. cum laude in human movement sciences and high-performance coaching.
He has published more than 50 papers and patents at the intersection between physiology, health, technology, and human performance.
He is co-founder of HRV4Training, advisor at Oura, guest lecturer at VU Amsterdam, and editor for IEEE Pervasive Computing Magazine. He loves running.
Social:

Always great articles. As an aside, besides using your app for a long time now (Pro version) which is fantastic, I wanted your opinion on EliteHRV which I also use. Most times the two are nowhere near identical with HRV4Training displaying a far lower value.
I take two readings everyday, one after the other. I use a Polar H10. I’ve used both apps for several years in order to get longitudinal data about my values.
Just wondering if you’d proffer a reason for the differences?
Thank you!
Great insight from you and Sabah! Surprised about her findings, because I would think that fasting would increase stress on the body and HRV might dip a little. I haven't tested that on myself, because I don't do more than a 24 hour fast anymore. I do notice that having a lighter dinner supports better sleep & recovery, leading to a higher HRV and lower RHR.